
Content created by Office of Budget (OB)
Topics on this page: IHS Budget Overview | IHS Programs and Services | Fulfilling the Administration’s Commitment to Indian Country through the Indian Health Service | Prioritizing Access to Quality Health Care Services | Prioritizing Health Care Services | Supporting Indian Self-Determination
Indian Health Service (IHS)

The mission of the Indian Health Service is to raise the physical, mental, social, and spiritual health of American Indians and Alaska Natives to the highest level.
IHS Budget Overview
(Dollars in millions)
| Services | 2014 /1 | 2015 | 2016 | 2016 +/- 2015 |
|---|---|---|---|---|
| Clinical Services: | 4,142 | 4,303 | 4,545 | +242 |
| Purchased/Referred Care (non-add) | 879 | 914 | 984 | +70 |
| Medicaid (non-add) | 738 | 771 | 781 | +10 |
| Preventive Health | 147 | 154 | 163 | +9 |
| Contract Support Costs | 612 | 663 | 718 | +55 |
| Tribal Management/SelfGovernance | 6 | 8 | 8 | -- |
| Urban Health | 41 | 44 | 44 | -- |
| Indian Health Professions | 28 | 48 | 48 | -- |
| Direct Operations | 66 | 68 | 68 | -- |
| Diabetes Grants | 147 | 150 | 150 | -- |
| Subtotal, Services | 5,190 | 5,438 | 5,744 | +306 |
| Facilities | 2014 /1 | 2015 | 2016 | 2016 +/- 2015 |
|---|---|---|---|---|
| Health Care Facilities Construction | 85 | 85 | 185 | +100 |
| Sanitation Facilities Construction | 79 | 79 | 115 | +36 |
| Facilities and Environmental Health Support | 211 | 220 | 227 | +7 |
| Maintenance and Improvement | 62 | 62 | 98 | +36 |
| Medical Equipment | 23 | 23 | 24 | +1 |
| Subtotal, Facilities | 460 | 468 | 648 | +180 |
| IHS Budget Totals – Less Funds From Other Sources | 2014 /1 | 2015 | 2016 | 2016 +/- 2015 |
|---|---|---|---|---|
| Total, Program Level | 5,649 | 5,906 | 6,392 | +486 |
| Health Insurance Collections /1 | -1,060 | -1,106 | -1,131 | -25 |
| Rental of Staff Quarters | -8 | -8 | -9 | -1 |
| Diabetes Grants /2 | -147 | -150 | -150 | -- |
| Total, Budget Authority | 4,435 | 4,642 | 5,103 | +461 |
Table Footnotes
1/ This column reflects the FY 2014 reprogramming of funds within the Services appropriation for contract support costs.
2/ These mandatory funds were pre-appropriated in P.L. 112-240, the American Taxpayer Relief Act of 2012, and P.L. 113-93, the Protecting Access to Medicare Act of 2014, and are proposed for reauthorization in FY 2016.
Full Time Equivalents
2014: 15,244
2015: 15,803
2016: 15,860
2016 +/- 2015: +57
IHS Programs and Services
The FY 2016 Budget requests $6.4 billion for the Indian Health Service (IHS), an increase of $486 million above FY 2015 and 49 percent above FY 2008. The President’s visit to the Standing Rock Reservation in 2014 reaffirmed the Administration’s commitment to address health disparities in Indian Country. The FY 2016 Budget requests increases for targeted areas where funding will have long-term impacts on the health and well-being of those served by IHS. Specifically, the Budget includes increased investments for the Purchased/Referred Care Program and other direct health care services to cover increases in costs due to medical inflation, population growth, and pay costs; proposes funding for staffing and operating costs for new and replacement tribal and IHS health care facilities; proposes substantial investments in IHS health care facilities; includes an increase for Health Information Technology to help modernize IHS systems; and includes funding to help improve collections from public and private insurance at IHS and tribally operated facilities, which are vital to a facility’s success. The Budget supports tribes and tribal organizations that administer health programs by fully funding estimated Contract Support Costs, and proposes a long-term solution for the Contract Support Costs program that would begin in FY 2017.
Fulfilling the Administration’s Commitment to Indian Country through the Indian Health Service
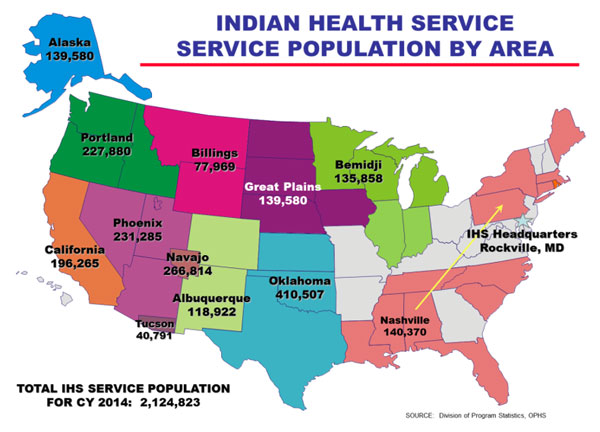
The IHS strives to assure that comprehensive, culturally acceptable personal and public health services are available and accessible to almost 2.2 million eligible American Indians and Alaska Natives who are members of 566 federally recognized tribes across the United States.
Tribal partnerships ensure that appropriate, culturally competent care is a focus for programs that impact tribal communities directly. To achieve this goal, IHS both serves as a health care system and partners with tribes as authorized by the Indian Self-Determination and Education Assistance Act, to provide health care and facilities services. Under this system, IHS and its tribal partners provide primary health care, behavioral health care, and community health services.
Additionally, IHS provides public health services that extend beyond the provision of health care. In partnership with other federal agencies, IHS builds sanitation systems to provide safe water and waste disposal for Indian homes, supports tribal self-governance and consultation, and recruits health professionals to serve in areas with high provider need through its Scholarships and Loan Repayment programs.
Prioritizing Access to Quality Health Care Services
IHS provides direct care services in over 650 hospitals, clinics, and health stations on or near Indian reservations. These facilities are managed by IHS, urban Indian health programs, and contracting and compacting tribes across the United States who provide services directly to tribal members, ensuring each tribe the opportunity to provide care in the best way possible for its members.
Construction: Construction projects are integral to ensuring continued access to quality health care services for Native people. Since the beginning of the Administration, IHS has worked to decrease construction backlogs by funding additional facilities through both the American Recovery and Reinvestment Act, and the annual IHS Budget. The FY 2016 Budget includes an additional $171 million over FY 2015 for a number of construction projects within IHS. These funds will allow IHS to build new health care and sanitation facilities, and repair and improve currently-owned structures to ensure access for American Indians and Alaska Natives across Indian Country.
Tribal Behavioral Health Initiative
IHS and Substance Abuse and Mental Health Services Administration will make investments in behavioral health as part of the Administration’s Generation Indigenous Initiative, created to remove the barriers to success for Native youth. As part of Generation Indigenous, IHS will dedicate resources to a new behavioral health effort that focuses on youth by expanding the successful Methamphetamine and Suicide Prevention Initiative. Through this $25 million expansion, IHS will provide funding to hire child and adolescent behavioral health providers to provide critical mental health services including prevention and early intervention of youth suicide and substance abuse.
The largest portion of this funding, $185 million, will be used to complete construction of the Gila River Southeast Health Center in Chandler, Arizona, and to design and initiate construction on the Salt River Northeast Health Center in Scottsdale, Arizona, the Rapid City Health Center in Rapid City, South Dakota, and the Dilkon Alternative Rural Health Center in Dilkon, Arizona. Once completed, these facilities are projected to collectively serve a user population of 59,504 patients.
IHS will also continue to work on improving sanitation facilities for American Indians and Alaska Natives. Many homes on tribal lands lack water or adequate sewage facilities. Throughout the course of the Administration, approximately 180,000 homes will have received sanitation facilities services for the first time or upgrades to existing services. The $115 million requested for FY 2016, in addition to partnerships with the Environmental Protection Agency, will allow IHS to make continued progress toward reducing the remaining backlog over the coming year.
Staffing New and Replacement Health Facilities: The Joint Venture Program links tribal and IHS funding to ensure construction and staffing of safe, state-of-the-art facilities for American Indians and Alaska Natives. Through this arrangement, IHS requests funds from Congress for staffing, equipping, and operating the facility while the participating tribe funds the costs of design and construction. These partnerships, where staffing costs have been funded by Congress in recent years, are key to increasing access to care and decreasing health disparities faced in Indian Country. The Budget includes an additional $18 million to support staffing and operating costs for three new or replacement health facilities to be completed by FY 2016, successfully funding the remaining facilities that were approved through the previous Joint Venture application process. When fully operational, these three facilities are projected to collectively serve a user population of over 16,844 patients. Additionally, IHS reopened another round application for the Joint Venture program based on significant tribal interest in this successful program.
Prioritizing Health Care Services
The Budget includes an increase of $306 million to support and expand the provision of health care services and public health programs for American Indians and Alaska Natives. Increased funding, the Affordable Care Act, and the permanent reauthorization of the Indian Health Care Improvement Act strengthened the provision of health care services for American Indians and Alaska Natives. However, despite tremendous progress, disparities remain. For example, the rates of drug-induced deaths as well as suicide rates remain elevated across Indian Country. Continued funding increases for health care services, like the increase that is part of the government-wide Generation Indigenous effort, are essential to reducing these disparities and ensuring healthier tribal communities.
Increases for Direct Healthcare Services: The Budget includes an increase of $147 million to cover increased costs associated with medical inflation, population growth, and pay cost increases for medical workers. Increases for direct healthcare services benefit all American Indians and Alaska Natives by ensuring continued health care service levels despite rising health care costs. The Budget also proposes reauthorization of the Special Diabetes Program for Indians, which provides grants to IHS, tribes, and urban Indian health programs to prevent and treat diabetes. The Diabetes Program has significant tribal support, and has been successful in achieving better health outcomes.
Purchased/Referred Care: The Budget includes $984 million, an increase of $70 million or 8 percent over FY 2015, for the Purchased/Referred Care program. IHS provides care both directly and by contracting with hospitals and other health care providers to purchase care when IHS and tribally-contracted programs are unable to provide care through internal networks. The Purchased/Referred Care program is often cited as the top tribal priority because it ensures access to health care services for eligible American Indians and Alaska Natives.
By using a medical priority review system, facilities determine preference for purchasing care when funding is limited. A 70 percent increase since FY 2008 has ensured that many programs can now pay for additional priorities beyond emergent services care. The requested FY 2016 funding increase ensures IHS can continue this expansion despite rising system-wide costs and a growing population.
Long-Term Solution for Contract Support Costs
Starting in FY 2017, contract support costs are proposed as a mandatory appropriation. This change would provide a long-term solution for funding of contract support costs, and would protect health care services provided to American Indians, Alaska Natives and Indian self-determination programs that improve the lives of America’s first people.
Health Insurance Reimbursements: In addition to funds included in this request, IHS estimates that in FY 2016, it will collect approximately $1.1 billion in health insurance reimbursements from Medicare, Medicaid, private insurers, and the Veterans Health Administration. Implementation of the Affordable Care Act expanded IHS’s ability to collect additional third-party health insurance reimbursements. By law, IHS is the payor of last resort, so it is essential that efforts are made to ensure the correct entity funds care provided to IHS eligible American Indians and Alaska Natives. This request includes an additional $10 million to improve collections from public and private insurance at IHS and tribally operated facilities. Third-party collections are crucial to hiring additional medical staff, purchasing equipment, making necessary building improvements, and ensuring accreditation standards are met.
Supporting Indian Self-Determination
Planning and delivery of health services at the local level often produces effective, quality health care because tribes and tribal organizations are the most knowledgeable about what services are needed in their communities. About 67 percent of the IHS budget is administered by tribes primarily through the authority provided to them under the Indian Self Determination and Education Assistance Act, which allows tribes to assume the administration of programs previously carried out by the federal government.
Contract Support Costs: The Budget fully funds estimated Contract Support Costs need at $718 million, an increase of $55 million above FY 2015. These funds are paid directly to tribes to support infrastructure needed to administer health programs and cover necessary costs in the operation of those programs. The estimated increase includes funding for new and expanded contracts and compacts. The Budget also requests a reclassification of contract support costs to a mandatory appropriation beginning in FY 2017. If enacted by Congress, this change is a long-term solution that will continue the policy to fully fund contract support costs, make new investments to ensure program integrity, and protect the health care services budget.
Investment Funding for Health Care Facilities Construction Projects
The FY 2016 Budget proposes an additional $172 million above FY 2015 for projects on the IHS Health Care Facilities Construction priority list, the Sanitation Facilities Construction priority list, and for much needed Maintenance and Improvement projects. The average age of IHS facilities is over 25 years, well above the industry standard for comparable private sector facilities of 9 to 10 years. To ensure facilities are safe for occupancy, IHS must spend additional funding on maintenance each year. These investments will decrease IHS's construction and maintenance backlogs across Indian Country and help ensure American Indians and Alaska Natives are receiving high-quality, state-of-the-art health care services.
Tribal Consultation: Recognizing that tribes are in the best position to understand the unique needs of their diverse communities, the President and other senior leaders have met with tribal leaders and groups both on Reservations and at the White House. Additionally, 2014 saw unprecedented communication on self‑determination issues between the federal government and tribal leaders, with IHS engaging in a robust plan, submitted to Congress, to ask for input from tribal leaders on possible long-term solutions for the Contract Support Costs program. IHS, in conjunction with other HHS agencies, intends to continue this communication via tribal consultation activities in FY 2016.
One of the largest consultations on the budget is the HHS annual, Department-wide Tribal Budget Consultation. At the beginning of each calendar year tribal leaders are provided an opportunity to communicate with all the operating and staff divisions of HHS. Tribal leaders are also able to exchange updated information, meet colleagues who face similar challenges, share their culture with other tribal members and HHS staff, and present recommendations for the IHS budget based on an annual tribal budget formulation process. Where possible, information shared with HHS is reflected in the FY 2016 Budget to ensure a continued legacy of improved health outcomes in Indian Country.